Nameless asked me in an email whether I had an idea of goals toward discharge, and whether I was being unexpectedly moved around and returned to my room (as his Mom was after hip surgery and found annoying.) Well, his Mom (and others who felt the same) must have impacted the standards of care.
Yesterday, here is the printout schedule I received (abbreviated):
OT 7:15-8:15 patient room
OT 8:15-8:45 patient room
PT 10:00-11:00 Gym (This was a sitdown lecture/roundtable on avoiding future falls)
PT 11:30-12:00 Gym
It all adds up to 3 hours, so I know it’s the full schedule – they have promised me three hours a day and no more (it may even be only 5 days a week.)
As far as goals toward getting out, that iis largely what they are working on shaping for me. The first PT workout Tuesday was exhausting, but it gave me a very clear idea of what they want me to be able to do. Some of it I can do now but need repetition to build strength and stamina – like walking with a walker around the gym. Tuesday I did it and it didn’t affect my oxygen but it skyrocketed my pulse. Yesterday I did it much more easily. (Interestingly, Tuesday also made it clear that my pulse going up presents as shortness of breath. But I digress.) Other tasks I can do but not in the target time frame. Still others – mostly those involving balance – not in this universe at this time (It’s not the fall – I have had balance issues my whole life. Of course the upside of that is that I have a pretty good idea of my limitations.) So specific goals are being formed, and I haven’t looked, but it would not surprise me if they are being slipped into the binder they gave me. And if not, I can probably request a copy. Also, at my leisure, the center’s TV system has about a dozen treatment-related videos, including one about what to expect on the discharge day.
I hope no one else here will ever need to go to rehab. But if you do, I hope this will help you have an idea what to expect, and mitigate any fear or nervousness. And the staff have been great (sure, some are better than others,and sure, some of them, being demanding is their job, so they are not going to seem as warm as others. But they are good at what they do.)
This is all for today, other than reading and rating comments (and responding to a few.) Today But rest assured I’m feeling good for the circumstances and getting better.
Today is the Marine Corps Birthday. Trinette has the day free after a long hard week of training and will be able to visit in daylight even in standard time. I shan’t be idle.
Click the picture for a guided tour
p. s. They also have an in-house psychologist! We just met, and I don’t think I’ll need her, but then I didn’t have surgery, so no mind numbing anesthesia, and besides I have Trinette and you all.
Yesterday, I was exhausted, and slept quite late. So I got busy putting this post together, and at a little before 8 p.m., I received an email informing me Margaret Atwood is having pacemaker surgery tomorrow, Wednesday. The link is to Substack, but if you are interested and don’t mind clicking the popup, you can find out more. She is due to turn 84 next month, and was only 12 whem she experienced her first extrasystole, and also she has a family history of Afib. I did see the episode of Impatient Griselda she alludes to, and no, I had no idea she was having an episode. But I take this seriously, however lightly she speaks of it. Although it’s unavoidable, I hate losing national treasures (even when it’s another nation – in this case, Canada.) And of course the pacemaker may well lenghthen her life significantly, so there’s that. I certainly hope it does.
Cartoon –
Short Takes –
Axios – Scoop: Marine Corps 3-star general advising Israeli military on Gaza ground operation
Quote – White House National Security Council spokesperson John Kirby told reporters at a briefing on Monday that there “are a few U.S. military officers with relevant experience to the operation the Israelis are conducting that are over there to share their perspective and to ask hard questions — the same hard questions we have been asking our Israeli counterparts since the beginning.” Click through for more. Here’s what I think is going on: Republicans (by whatever name) have much in common with children (particularly toddlers), and one of those commonalities is that, in order to persuade them to do something, you have to be able to get them to think it was their own idea. I could be wrong – but all that brain power looks like it to me.
The 19th – Tammy Baldwin has won big in closely divided Wisconsin. Can she do it again?
Quote – Baldwin is one of the country’s most progressive senators, and she’s running for a third term in what could be the country’s most closely divided state. She played a prominent role mobilizing Democratic voters ahead of a Wisconsin Supreme Court election this year that became a referendum on abortion rights. A lower court ruled this fall that abortions could resume in the state. Democrats believe that 2024 voters will remember the year in which their reproductive rights were in question; Republicans hope the ruling will diminish the issue’s salience next year. Either way, Baldwin also has a formidable track record of appealing to Wisconsin’s more rural, conservative pockets with her economic agenda — and she’s already busy talking to voters and raising money as she waits for a high-profile Republican challenger to enter the race. Click through for article. I’m old enough to remember when Wisconsin was pretty progressive overall, and I find it actually painful that that has been lost – and so acrimoniously at that. This is Scott Walker’s “legacy.” It needs to go – and I wish Baldwin every success.
Yesterday was strange – not that nothing happened around the nation and the world, but that so many of the things that did happen were so odd. We can blame climate change for some of it, but not for all, certainly. I think I remember that Colleen’s delayed surgery was for carpal tunnel or somethiing of the sort – if so, she may be recovering just fine but not feel up to commenting yet. I hope that’s the case, but also hope to hear soon.
Cartoon
Short Takes – News of the Weird today!
WFAA – ‘Once you see one, you’ll see another’: Have you seen one of these worms in your yard? They’re toxic. Here’s how you deal with them.
Quote – “The way this flatworm harms our ecosystem is it eats earthworms, which are necessary for our forests, our crops…our gardens to survive,” Morgan-Olvera said, “In order for it to digest earthworms, it secretes a chemical, or a neurotoxin, and that can cause an allergic reaction on your skin if you’re handling it.” Click through for full story, including what – and what not – to do.
NBC News – Vehicles stuck on Detroit freeways after torrential downpour
Quote – [I]t was predicted that the city would get close to two inches of rain Friday night, but nearly seven inches fell. “The intensity of these storms exceeded the design standards for pump stations and combined sewer overflow facilities serving the Detroit region,” Brown said at a press conference on Saturday. There was so much rain that there was nowhere for the water to go, he explained, other than flooding streets and basements. Click through for more. (But there’s no such thing as climate change. Right.)
NextShark – Australian Woman Who Woke Up From Surgery With Irish Accent May Be Stuck With It for Life
Quote – This week, Yen underwent a brain scan which confirmed “nothing wrong.” But she was diagnosed with Foreign Accent Syndrome (FAS), a rare medical condition that may be triggered by neurological or psychological damage, according to speech pathologist Kirrie Ballard. “Foreign Accent Syndrome is a legitimate disorder. It’s described as a person’s speech changing, so that it sounds as though they’re speaking in a different accent to their habitual accent,” Ballard told 60 Minutes. Click through for the story. Bizarre, but true. And it says a lot about how we humans treat each other – none of it good.
Experts in autocracies have pointed out that it is, unfortunately, easy to slip into normalizing the tyrant, hence it is important to hang on to outrage. These incidents which seem to call for the efforts of the Greek Furies (Erinyes) to come and deal with them will, I hope, help with that. As a reminder, though no one really knows how many there were supposed to be, the three names we have are Alecto, Megaera, and Tisiphone. These roughly translate as “unceasing,” “grudging,” and “vengeful destruction.”
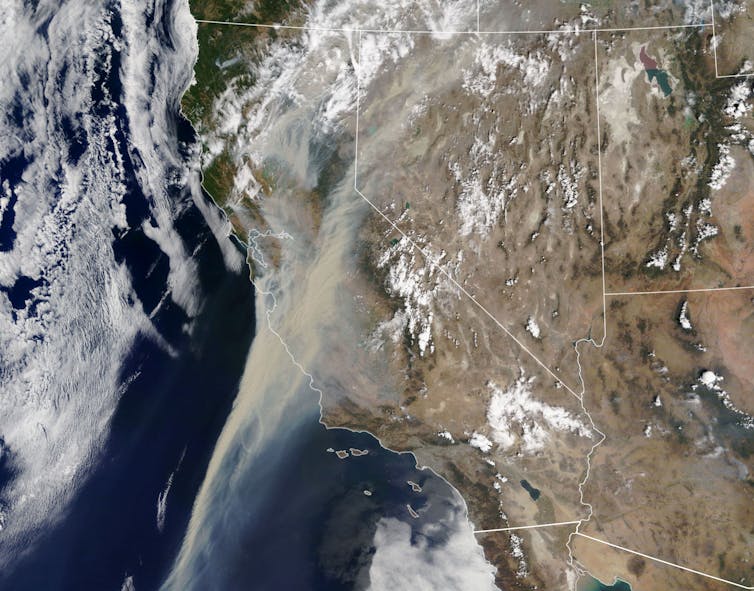
Not everywhere in the United States is experiencing wildfires this year – yet. But just because you cannot see it or even smell it does not mean it is not dangerous to you – and I don’t mean just indirectly. We need to be aware as much as we can.
================================================================
What’s in wildfire smoke, and why is it so bad for your lungs?
The health impact of wildfire exposure depends in part on the fire itself and how much smoke a person breathes in, how often and for how long. AP Photos/Noah Berger
If I dare to give the coronavirus credit for anything, I would say it has made people more conscious of the air they breathe.
A friend texted me recently after going for a jog in the foothills near Boise, Idaho, writing: “My lungs are burning … explain what’s happening!!!”
A wildfire was burning to the east of town – one of hundreds of fires that were sending smoke and ash through communities in hot, dry western states. As an environmental toxicologist, I research how air pollution, particularly wood smoke, impacts human health and disease.
I gave my friend the short answer: The state had issued a yellow, or moderate, air quality index warning due in part to wildfires. The high temperature for the day was expected to reach 100 degrees Fahrenheit, and it was already approaching 90. That combination of high temperatures and elevated levels of particles from a fire can affect even healthy lungs. For someone with lung damage or respiratory illness, moderate levels of smoke particulate can exacerbate respiratory problems.
That’s only the start of the story of how wildfire smoke affects humans who breathe it. The rest, and how to stay healthy, is important to understand as the western wildfire season picks up.
What’s in wildfire smoke?
What exactly is in a wildfire’s smoke depends on a few key things: what’s burning – grass, brush or trees; the temperature – is it flaming or just smoldering; and the distance between the person breathing the smoke and the fire producing it.
The distance affects the ability of smoke to “age,” meaning to be acted upon by the sun and other chemicals in the air as it travels. Aging can make it more toxic. Importantly, large particles like what most people think of as ash do not typically travel that far from the fire, but small particles, or aerosols, can travel across continents.
Smoke from wildfires contains thousands of individual compounds, including carbon monoxide, volatile organic compounds (VOCs), carbon dioxide, hydrocarbons and nitrogen oxides. The most prevalent pollutant by mass is particulate matter less than 2.5 micrometers in diameter, roughly 50 times smaller than a grain of sand. Its prevalence is one reason health authorities issue air quality warnings using PM2.5 as the metric.
The human body is equipped with natural defense mechanisms against particles bigger than PM2.5. As I tell my students, if you have ever coughed up phlegm or blown your nose after being around a campfire and discovered black or brown mucus in the tissue, you have witnessed these mechanisms firsthand.
The really small particles bypass these defenses and disturb the air sacks where oxygen crosses over into the blood. Fortunately, we have specialized immune cells present in the air sacks called macrophages. It’s their job to seek out foreign material and remove or destroy it. However, studies have shown that repeated exposure to elevated levels of wood smoke can suppress macrophages, leading to increases in lung inflammation.
What does that mean for COVID-19 symptoms?
Dose, frequency and duration are important when it comes to smoke exposure. Short-term exposure can irritate the eyes and throat. Long-term exposure to wildfire smoke over days or weeks, or breathing in heavy smoke, can raise the risk of lung damage and may also contribute to cardiovascular problems. Considering that it is the macrophage’s job to remove foreign material – including smoke particles and pathogens – it is reasonable to make a connection between smoke exposure and risk of viral infection.
Recent evidence suggests that long-term exposure to PM2.5 may make the coronavirus more deadly. A nationwide study found that even a small increase in PM2.5 from one U.S. county to the next was associated with a large increase in the death rate from COVID-19.
Wildfire smoke pours over palm trees lining a street in Azusa, Calif., on Aug. 13, 2020. AP Images/Marcio Jose Sanchez
What can you do to stay healthy?
The advice I gave my friend who had been running while smoke was in the air applies to just about anyone downwind from a wildfire.
Stay informed about air quality by identifying local resources for air quality alerts, information about active fires, and recommendations for better health practices.
If possible, avoid being outside or doing strenuous activity, like running or cycling, when there is an air quality warning for your area.
Be aware that not all face masks protect against smoke particles. In the context of COVID-19, the best data currently suggests that a cloth mask benefits public health, especially for those around the mask wearer, but also to some extent for the person wearing the mask. However, most cloth masks will not capture small wood smoke particles. That requires an N95 mask in conjunction with fit testing for the mask and training in how to wear it. Without a proper fit, N95s do not work as well.
Establish a clean space. Some communities in western states have offered “clean spaces” programs that help people take refuge in buildings with clean air and air conditioning. However, during the pandemic, being in an enclosed space with others can create other health risks. At home, a person can create clean and cool spaces using a window air conditioner and a portable air purifier.
The EPA also advises people to avoid anything that contributes to indoor air pollutants. That includes vacuuming that can stir up pollutants, as well as burning candles, firing up gas stoves and smoking.
================================================================ Alecto, Megaera, and Tisiphone, “can travel across continents” – I suppose there are things scarier than that, but not many, and not much. Although “can suppress macrophages” is also right up there. At least this article gives us some practical, personal advice on avoiding as much damage as possible – and you can’t do it for us; we must practice it ourselves. I think the best thing you can do for us at this point is to help inspire people to VOTE, and specifically to VOTE BLUE, no matter who, top to bottom. And then hang around for the fights which are certain to come, and help us prevail. Only then will we be able to start the real battle to prevent the end of the world as we know it.
Experts in autocracies have pointed out that it is, unfortunately, easy to slip into normalizing the tyrant, hence it is important to hang on to outrage. These incidents which seem to call for the efforts of the Greek Furies (Erinyes) to come and deal with them will, I hope, help with that. As a reminder, though no one really knows how many there were supposed to be, the three names we have are Alecto, Megaera, and Tisiphone. These roughly translate as “unceasing,” “grudging,” and “vengeful destruction.”
I feel the need to share this because, although unrelated to current events, it is profoundly accurate – and it is something I never expected to see, hear, read, in my lifetime. It is jaw-dropping.
================================================================
A doctor’s open apology to those fighting overweight and obesity
Doctors have told people who are overweight to exercise more and eat less, when in fact their overweight may be due to genetic or other factors that exercise won’t change. UConn Rudd Center for Food Policy & Obesity, CC BY-SA
Obesity has emerged as a significant risk factor for poor outcomes in patients infected with COVID-19. Based on how doctors and others in health care have previously treated patients with obesity or overweight conditions, my guess is that many will respond by declaring: “Well, it’s their own fault for being overweight!”
In the spirit of recognizing that people who struggle with weight loss include our family and friends, let me propose a different sentiment.
To those who we have shamed for having excess body weight and/or failing diets: “You were right, and we are sorry. After giving you undoable tasks, we ridiculed you. When you tried to tell us, we labeled you as weak and crazy. Because we didn’t understand what you were experiencing, we looked down on you. We had never felt it ourselves. We did not know. And for that, we apologize.”
This is just one version of the apology we owe our fellow human beings whom we told to lose weight using diet and exercise. Then, when it didn’t work, we blamed them for our treatment plan failures and smothered their feedback with prejudice and persecution.
As a physician and researcher, I have worked in this space for many years. I have witnessed firsthand the life-altering power of preexisting ideas, judgments and stereotypes. I have seen how unfounded, negative ideas are woven through virtually every interaction that those struggling with weight loss endure when seeking help.
And there are tens of millions of them. The Centers for Disease Control and Prevention classifies more than 70% of U.S. adults as overweight, and more than 40% as obese. Those numbers continue to climb, and even when some manage to lose weight, they almost always gain it back over time.
Rash judgments
To illustrate, imagine that I am your doctor. You have a body rash (which represents the condition of being overweight or obese), and you make an appointment with me to discuss a treatment plan.
During your visit, my office staff uses stigmatizing language and nonverbal signals that make it clear we are annoyed at the idea of dealing with another rash person. We invoke a set of assumptions that dictate the tone of our relationship, including the notions that you are lazy or ignorant or both. You will sense my disgust, which will make you uncomfortable.
Unfortunately, health care providers commonly treat patients who struggle with weight loss by assigning stereotypes, snap judgments and ingrained negative attributes – including laziness, noncompliance, weakness and dishonesty.
After this uncomfortable exchange, I will prescribe a treatment program for your rash and explain that it’s quite straightforward and easy to use. I will point you to several resources with pictures of smiling people with beautiful skin who never had a rash to emphasize how wonderful your outcome will be. “It’s just a matter of sticking to it,” I will say.
Back at home, you are excited to start treatment. However, you quickly realize that putting on the cream is unbearable. It burns; your arms and legs feel like they’re on fire shortly after you apply the treatment. You shower and wash off the cream.
A dismal conversation
After a few days, you try again. Same result. Your body will not accept the cream without intolerable burning and itching. You return to my office, and we have the following conversation:
You: Doctor, I cannot stick to this plan. My body cannot tolerate the cream.
Me: This is exactly why doctors do not want to deal with rash people. I’m giving you the treatment and you won’t stick to it. I put the cream on myself every morning without an issue.
You: But you don’t have a rash! Putting this cream on when you have a rash is different than putting it on clear skin. I do want to get rid of my rash, but I cannot tolerate this cream.
Me: If you don’t want to follow the treatment, that’s up to you. But it’s not the cream that needs changing. It is your attitude toward sticking with it.
This exchange illustrates prejudical behavior, bias and a disconnect between a provider’s perceptions and a patient’s experience.
For someone who wants to lose weight, the experience of a diet and exercise prescription is not the same as for a lean person on the same program. Perceiving another person’s experience as the same as one’s own when circumstances are different fuels prejudice and bias.
That night, though, you can’t help but wonder: “Is something wrong with me? Maybe my genes or thyroid or something? The cream seems so fun and easy for everyone else.”
At this point, the blame unconscionably lands on the patient. Despite an undeniable explosion of this rash, and abysmal treatment adherence rates while we have been touting the cream, we stubbornly maintain it works. If the rash is expanding, and hundreds of millions of people are failing treatment or relapsing every day, well – it’s their own fault!
As time goes on, you feel increasingly discouraged and depressed because of this untenable situation. Frustration wears on your sense of optimism and chips away at your happy moments. You have this rash and you can’t tolerate the treatment plan, but no one believes you. They judge you, and say you choose not to use the cream because you lack willpower and resolve. You overhear their conversations: “It’s her own fault,” they say. “If that were me, I would just use the d#$% cream.”
This is the very definition of prejudice: an opinion, often negative, directed toward someone and related to something that the individual does not control. Although it has been extensively demonstrated that the causes for overweight and obesity are multifactorial, the myth that it’s the patient’s fault is still widely accepted. This perception of controllability leads to the assignment of derogatory stigma.
A setup for failure
That evening you sit alone. You think there’s not a single person on the planet who believes your body won’t tolerate this treatment. Society believes you brought this on yourself to begin with; there doesn’t seem to be a way out.
We have driven those with overweight and obesity conditions to this place far too many times. We have set them up to take the fall for our failed treatment approaches. When they came to us with the truth about tolerability, we loudly discredited them and said they were mentally weak, noncompliant or lazy.
So where do we go from here? If we agree to stop stigmatizing, stereotyping and blaming patients for our treatment failures, and we accept that our current nonsurgical paradigm is ineffective – what takes its place?
For starters, we need a new approach, founded on respect and dignity for patients. A fresh lens of acceptance and suspended judgment will allow us to shift our focus toward treatments for the body, rather than “mind over matter,” which is a concept we use for no other medical condition. A perspective based in objectivity and equality will allow caregivers to escape the antiquated blaming approach and perceive those with overweight or obese conditions in the same light as those with other diseases. Only then will we finally shift the paradigm.
================================================================ Alecto, Megaera, and Tisiphone, I point out that The Conversation operates on a Creative Commons license (material is free to share, with attribution), and I hope everyone will feel free to share this. I wish someone would share it with Bill Maher (and then we would see how actually committed he is to science over prejudices, wouldn’t we.) You ladies can spread it too. Thanks.